What Is A Xanthelasma?

The appearance of a Xanthelasma is a yellow or white flat plaque or spot over the upper or lower eyelid, most often near the inside of the eye. They are made up of cells, that eat up blood fats. A Xanthelasma is therefore essentially a fatty cholesterol deposit around the eye. They do occur in other parts of the body, but they would then be called Xanthoma.
How can a Xanthelasma be removed?
Please read the sections below before booking. Xanthelasma treatment is usually straightforward, but the most suitable method depends on your eyelids, and recurrence and scarring are important to understand.
Different terms for Xanthelasma = Xanthoma = Cholesterol on eyelid = Fatty Deposit Eyelid = Fatty Lump around the eye = White Spot around the eye = Eye Cysts = Yellow marks on eyelid = Yellow eyelids = Yellow eyelid marks = Yellow Eyelid Bump = Eyelid cholesterol = Cholesterol deposits on eyelids = Yellow patches on eyelids = Fatty deposits on eyelids = Xanthoma around the eyes
What is xanthelasma
Xanthelasma are soft, yellowish or whitish plaques that sit in the skin of the eyelids, most often near the inner corner. They are made of lipid-laden cells (cholesterol-type deposits).
They are harmless and benign. They are not an infection, not skin cancer, and not contagious. People seeking treatment do so for cosmetic reasons, or because the plaques are slowly enlarging.
You may also see the word xanthoma. That term is often used for similar deposits elsewhere on the body, while xanthelasma refers specifically to the eyelids.
How Can I Self Diagnose A Xanthelasma?
The appearance is usually beyond doubt, because there are not many other known conditions causing yellow plaques in the same areas. Another small tumour around the eyes called Syringoma can sometimes be confused with it. Sometimes there can also be cysts which look similar although they tend to be bulkier.
Who gets Xanthelasma?
Xanthelasma are more common in mid-life and later adulthood, often appearing in people in their 40s or 50s, but they can occur earlier.
They are reported slightly more often in women than in men. Some people have a family tendency. Others develop them without any obvious trigger. Some patients have reported triggers like pregnancy and other life events.
Some patients have raised cholesterol or other lipid abnormalities. Many do not.
What causes them and how can I prevent Xanthelasma growing bigger or re-forming after removal?
There is no guaranteed way to prevent xanthelasma. Some people develop them even with cholesterol levels in the normal range, and some people with high cholesterol never develop them at all.
That said, xanthelasma are often associated with lipid metabolism and cardiovascular risk factors, and there is good evidence that xanthelasma can be a marker of vascular risk in some people.
Practical prevention is therefore less about a cream or a local eyelid treatment, and more about general health measures:
checking cholesterol and other lipids
addressing cardiovascular risk factors (blood pressure, smoking, diabetes, weight, exercise)
following your GP’s or lipid clinic advice if treatment is indicated
Even when cholesterol is well controlled, xanthelasma can still recur. But from a health point of view, cholesterol optimisation is still worthwhile.
Do they get bigger? Will they go away on their own? How about creams?
In most cases, established xanthelasma do not disappear spontaneously. They often stay stable for long periods, but they can also enlarge slowly.
Creams do not reliably remove xanthelasma. Cholesterol treatment is mainly aimed at reducing cardiovascular risk, not at treating the eyelid plaques. Some patients do report that plaques soften, shrink, or stop progressing once lipid treatment is optimised, but this is not reliable enough to be considered a treatment we can recommend at this point. You can try just taking statins and see what happens, but results may be disappointing. What statins often do, though, is to stop Xanthelasmas from growing further.
If the plaques bother you cosmetically, removal is usually the most predictable option.
Health considerations and cholesterol management
Xanthelasma are harmless in themselves, but they can sometimes act as a visible “shop window” into what is happening in the arteries.
There is published evidence that people with xanthelasma can have a higher risk of cardiovascular disease, and this may apply even when a standard cholesterol test looks acceptable. In other words, xanthelasma can be a reason to take cardiovascular risk review seriously rather than to ignore it.
What we usually recommend:
ask your GP for a cholesterol and lipid profile if you have not had one recently
consider a broader cardiovascular risk assessment, especially if you have other risk factors
if you are already on cholesterol treatment and your xanthelasma recur or new plaques appear, it is sensible to review whether lipid control is optimal and whether you need a medication adjustment or a lipid specialist opinion
This is not about scaring people. Many patients are perfectly well. It is simply good preventive medicine.
What Can Thames Valley Surgical Services Do For Me?
Scarring
Firstly, a word of warning. All Xanthelasma treatments will leave scars and, depending on the healing process, the scar may be better or worse. However, on many occasions the scars are almost unnoticeable, particularly when a Xanthelasma is excised. Excision can also remove a small amount of redundant eyelid tissue in patients whose eyelids are no longer quite so taut, which may be an additional benefit.
We audit our figures and about 5–10% of our patients treated with electrodessication need a repeat treatment. Rarely, patients are not happy with the degree of improvement achieved. Electrodessication is the simpler and quicker treatment, and if you are not happy with the cosmetic result, the area can still be excised later.
A habit to return…
Please also be aware that Xanthelasmas have the unfortunate habit of returning, whichever treatment you choose. The lower your cholesterol, the less likely a return appears to be. Around 50% of patients seem to be clear for a long period of time, while the other 50% may need further treatment within months or 1–2 years.
A recent learning point is that, in people with hay fever, it may be better to wait until after the hay fever season. Some swelling is to be expected after treatment, and this can be exacerbated by hay fever and eye rubbing. Swelling can last for up to two weeks, although improvement is usually much quicker.
When you come for your consultation, I will talk to you about cholesterol management, as your eyelids can be the “shop window” to your heart. I believe every Xanthelasma patient should be properly assessed for lipid management. Action now may help prevent problems many years down the line. Sometimes I spend more time discussing lipid management than the procedure itself.
Option 1: Microcautery = Electrodessication (fast and quick, 80% improvement, cheaper)
Microcautery is a controlled method of treating the plaque without cutting it out. It is usually quick and does not require stitches.
In our experience, this typically leads to a clear cosmetic improvement. Some patients need a second session for small residual areas. If a second or third treatment is needed within a defined time window, we discount it, because sometimes staged treatment is the safest way to protect the eyelid skin.
Microcautery is often a good option when:
plaques are small to moderate in size
the lesion is superficial
the patient prefers no stitches
we want a controlled, staged approach
Expected healing: local swelling and redness are common. The eyelids are sensitive and they can swell more than people expect.
A practical real-world point: if you suffer from hay fever and rub your eyes in spring, it is often better to plan treatment outside peak allergy season. Eye rubbing can increase swelling and prolong the recovery phase.
Repeat Treatment Cost
Please note that repeat treatments will incur additional costs. Around 90% of patients complete their treatment within the price outlined on this page, but a small proportion will require one or more further sessions.
We offer a 50% “no profit” discount on second or third treatments. However, we are a private clinic and must cover our costs.
If, after treatment, you require excision of a residual area or a scar revision, this would involve an additional charge.
Option 2: Full surgical removal of Xanthelasma (better result i.e. 99% improvement and very fine line mostly invisible scar)
This option is limited to patients with small to medium-sized Xanthelasmas (they can be long, but not too large in diameter), because removing too much eyelid tissue may leave the skin too tight. There needs to be enough excess or redundant skin for this option to be safe.
For that reason, excision is usually more suitable in older patients. Younger patients with very taut skin may experience problems after surgery if too much tissue is removed, as the eyelid can become tight.
If the stitches were to come apart (for example due to swelling from hay fever, rubbing, allergy or infection), a worse scar than with electrodessication could result. The scar may be deeper, and because part of the eyelid skin has already been removed, secondary scar revision may not always be straightforward. This is a theoretical risk and it rarely happens, but it is important to understand.
In addition, the shape of the eyelid can change slightly because skin is removed on one side but not the other. In most older patients this settles and stretches out over time, but it may be more noticeable in younger patients.
That said, I have not experienced patients complaining about any of the above issues. Very rarely do we have unsatisfied patients; most are very happy with the outcome.
Prior to surgery we will give you a local anaesthetic, usually via injection.
Alternatives to the Treatments we provide
Do nothing
This may not sound an attractive option for a person already researching treatments, but as Xanthelasma are benign, many people live with them and never treat them.
Try a statin (cholesterol lowering tablet) first
Sometimes people start a statin and the Xanthelasmas may disappear. But keep in mind this is mainly about reducing cardiovascular risk. It can sometimes slow progression, and occasionally plaques may reduce, but it is not a reliable cosmetic treatment.
Different methods
Different clinics offer different methods. Methods include Yag Laser, Acid, Freezing and more. Some websites make outlandish promises: “Our method is the best” or “Our method is the safest”. Truth is, what matters most is the experience of the person doing the surgery with the equipment they use. Often they try to sell you very expensive treatments when the same can be achieved less expensively.
Dr Kittel: Here is my opinion on other methods:
(Yag) Laser
I believe this to be a good method if operated by an experienced operator. The key is operator skill, appropriate settings, and understanding eyelid anatomy. It is not cheap due to equipment being expensive and the fact multiple sessions may be needed. Yag laser has been compared to acid treatment and found similarly effective for smaller and more effective for thicker lesions. Several applications may be required. It has a good safety profile
Chemical Cautery = Acid Treatment
Inexpensive and successful in a not insignificant number of patients if the person doing it is experienced, but Acid very close to the eye is something I have not been entertaining. If it gets into the eye it could be very damaging and it only takes the patient sneezing etc…
Cryotherapy (freezing)
You have to freeze the tissue underneath to have the Xanthelasmas falling off, which I think is quite dangerous due to the underlying structures like the tear canals. Also, it may carry a higher risk of pigment change or scarring on delicate eyelid skin. So again, if someone is very experienced then I think it may be a good method for them, but I have never entertained this as it is too crude a method for me.
How to “spot a dud”
Most services are very good at what they do and will help you and offer treatments that you are able to trust. However, when choosing a treatment I would always assess the following:
- Does the website over-promise the “best method”? Do they provide scientific evidence and papers for their claim?
- They promise “no scars” or “guaranteed no recurrence”
- They rely heavily on marketing words rather than showing realistic healing and outcomes
- They do not discuss recurrence or trade-offs
- They do not ask about cholesterol or advise a GP check
- Do they try to scare you away from a treatment quoting side effects like an “Ectropion” with excision when most people over 45 don’t mind loosing a bit of eyelid tissue and a few wrinkles. I have never have encountered this issue in my life as a surgeon.
- Do they try to sell you a “better” treatment at an astronomical price? Do they upsell expensive technology as if the device guarantees the result? It reminds me of red wine: Pay 10 times more to get a wine that may be 10% better than a reasonably priced wine. Sometimes you pay Millions for a bottle of red wine from the Titanic and when you open it it turns out to be vinegar.
- Do they offer one or several methods, do they have experience with different methods to make a claim on their best method or do they need to pay off expensive equipment they bought?
- Do they show you pictures of successful surgery. Do they also show what it looks like when a patient has to come back? Do they show a variety.
Don’t trust a service that shows you only great outcomes and makes huge promises until you see the consent form and have to consent to all sorts of reasonable or unreasonable side effects and possibilities. That shows you they are not magicians, either
Cost of Xanthelasma Removal: from £275*
Electrodessication = Microcautery of Xanthelasma
The cost of removal for Fatty Cholesterol Deposits around the eye (Xanthelasma) starts at £275* for one eyelid and £75 for every further eyelid, regardless of the size of the Xanthelasma. This does not include the consultation. For further price guidance click here
Furthermore, if you need a second or third treatment within 3 months of the first treatment we will provide this at 50% of the initial cost (i.e. say you had 2 Xanthelasmas for £410, you will pay £205 for a second treatment)
Full surgical removal of Xanthelasma:
Full cutouts are priced at £495 (£435 once consultation discount applied*) for the first Xanthelasma and £295 for every further Xanthelasma up to 2cm. More extensive Xanthelasmas are more expensive (but not hugely so). There are no discounts for further procedures because any further procedure is due to the natural re-occurence of Cholesterol in a new different area (which was not cut out).Xanthelasma stitches are very small and therefore harder to remove (not impossible). Stitch removal is therefore included in this price. However, we can, for the brave, also give you a free stitch removal kit or if you live far away your GP nurse may be able to help.
* consultation discount of £60 has been applied in this price
Make an appointment
If you would like treatment, the next step is a consultation so we can confirm diagnosis, discuss the best method for your eyelids, and go through realistic healing and outcomes. Please ensure you watch the video and read our patient information form in detail before the discussion. Make sure you have understood the content of this complete page, so we can have a good discussion with an informed patient.
If you live far away, you may still find this page helpful as a guide for what to ask and what to expect, even if you choose a different clinic.
Accessibility Information: Locations Appropriate for Referral or Treatment:
We provide Minor Surgery / Skin Surgery for Lipomas, Cysts, Warts, Moles, Skin Tags, Xanthelasmas and Split Earlobes in Maidenhead, Berkshire, which is near Windsor and Ascot and Heathrow Airport and close to London, South Buckinghamshire, South Oxfordshire, Hampshire and Surrey. TVSS are adjacent to Henley-On-Thames, Marlow, and Twyford. Also, we are close to Slough, Bracknell, Basingstoke, Egham and Gerrards Cross. Chalfont St Peter, Northolt, Harrow and Wembley. Rickmansworth, Richmond, Twickenham, Staines and Virginia Water. Sunningdale and Sunninghill, Ruislip, Reading, Wokingham and West Drayton. Uxbridge, Farnborough, Woking, Guildford. Oxford, Banbury, Milton Keynes and Coventry. Essex, Sussex, Kent, Swindon, Portsmouth and Bristol, Bath, Brighton, Eastborne and Southhampton are all no more than an 45 minutes to 2 hours away. Via the M4 we are also accessible to certain locations in South Wales
Example of Electrodessication Treatment
Below you can see more examples, healing patterns, and honest discussion of what can go wrong and how we manage it. This is detailed on purpose, because xanthelasma treatment is often oversimplified online. If you want to see real examples of healing, including less-than-perfect outcomes, see the case examples below

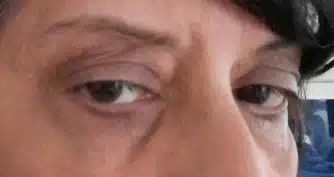
Xanthelasma in 47 year old patient
Upper eyelid of a 47 year old gentleman with a Xanthelasma. Dr Kittel saw him in January 2022 to treat him with Electrodessication treatment.

After Electrodessication Treatment
This is the scar remaining after Electrodessication treatment and this represents a typical scar. Some people have better scars, some are worse. Scars can sometimes be stronger, more pronounced or taking longer to heal. They also tend to be pink to start and then get whiter. If you pick them (the initial scabs) or they get infected, they may be worse. I saw him for repeated treatment of his other eyelid, see below. Note, the right lower eyelid had also been treated and had healed well, too, but is under the mask.

Same man left eyelid before treatment
This is the left upper eyelid of the same man. Dr Kittel treated his left upper eyelid in January too.

After 1 Xanthelasma treatment with Electrodessication – not fully resolved
The left upper eyelid had not fully resolved. At a distance the Cholesterol is already much less yellow (as only deeper Cholesterol remains), but it is not ideal. This man came for a second treatment of the left upper eyelid at 50% of the cost. The right upper eyelid (see above) and the right lower eyelid (hidden by mask above) were as good as we can get them and the patient was happy with the outcome.

This is a typical picture right after Electrodessication (this is the same patient as the 4 pictures above).
The swelling on the eyelid is the local anaesthetic. The bloody dot in the left upper corner is from the injection. The remaining Xanthelasma was fully treated and covered in brown iodine (to prevent infection). Subsequently the iodine is dried away. Within 2 days a scab will form and when the scab falls off you will know whether or not the treatment was successful. In this case Dr K had to choose a slightly higher energy setting to get the deeper layers and destroy the remaining Cholesterol. I will try to post further pictures when they become available.
Example of Excision Treatment 1

Xanthelasma in a 55 year old lady
This is the left upper eyelid of a 55 year old caucasian lady before treatment

6 months after full excision of Xanthelasma
This is a picture of the same left eye of the lady above 6 months after full excision of the Xanthelasma in March 2023 – see comment below
Scar is covered with make up
If you look carefully, there is actually a small scar in this lady. This scar is very discreet and can easily be covered with make up, but I thought it worthwhile pointing out for complete transparency.
Example of Excision Treatment 2

Xanthelasma in a 62 year old lady
These are both lower eyelids containing large and thick Xanthelasmas in January 2025

6 months after full excision of both lower eyelid Xanthelasma
These are pictures of the same ladies left and right lower eyelids 2 months after Xanthelasma removal. Scarring is discreet and hardly noticeable
Example of Excision Treatment 3

Upper eyelid Xanthelasma in Asian Gentleman
Both upper eyelids in a 53 year old asian gentleman before excision of the Xanthelasmas. I tend to recommend full excision to asian patients, because their Xanthelasmas tend to go deeper and the discolouration from the Electrodessication method is more visible.

6 weeks after excision
This is a picture of the same gentleman 6 weeks after excision. In fact he had the stitches on the left coming apart a little during recovery, yet still showed excellent healing. I often advise asian patients to start a Cholesterol tablets after excision.
Example of Excision Treatment 4

Xanthelasma before excision in 45 year old
This is the right upper eyelid of a 45 year old caucasian gentleman. He came and saw us in December 2022.

Scars 3 months after Xanthelasma excision
These are the scars remaining after excision of of all 3 Xanthelasmas excactly 3 months later in March 2023

Xanthelasma left eyelid
This is the left upper eyelid of the same man. You can see 2 Xanthelasmas on the lower eyelid, but also a few spots / milia, which we treated with Electrodessication

Left upper eyelid 3 months after Xanthelasma and milia treatment
This is the same man 3 months after completion of treatment. Overall he wrote to me how happy he was
Excision vs Electrodessication
| Excision | Electrodessication |
Price | Higher | Lower |
Speed | Takes time | Very quick |
Second procedure due to incomplete removal within 4 | Uncommon | 5-10% |
Improvement in looks (typical, not an individual | 95% | 80% |
Possible in under 45 year old | Not usually, unless very small | Yes, but satisfaction with the outcome cannot always be guaranteed. Not good for patients with darker skin. |
Stitches needed | Yes | No |
Chance of stitches coming apart | Yes | No |
Stitch removal needed | Yes | No |
Second procedure within 3 months (incomplete removal | No | Yes |
Guarantees Xanthelasma will not return | No | No |
Chance of significant bruising and bleeding | <5% | <1% |
Patient dissatisfaction | 2% | 8% |
Type of scar | Fine line | Same size as previous Xanthelasma |
Typical pain in recovery | Minor | Minor |
Recommended in darker skinned patients | Yes | It depends |
Recommended in lighter skinned patients | Yes | Yes |
Summary of our experience with Xanthelasma patients over the years:
No Xanthelasma treatment is perfect. In Electrodessication we have to go slowly and start with low energy settings to not damage the eyelid. this means, some patients have to return.
Electrodessication is a heat based treatment similar to cautery, laser etc. Therefore caution and experience is required.
We see a good number of patients that have been to other services and had no success with a treatment.
An alternative treatment we do not offer is the treatment with Tricloracetic Acid, the most common side effect here is hypopigmentation of the skin and you are more likely to need repeat treatments. See here: https://pubmed.ncbi.nlm.nih.gov/19617785/
It is very important that your expectations are realistic. It is also important you understand that new Cholesterol can form. If it forms within the scar it is usually speckled and previous treatment can often be recognised. The stronger the scar the less likely Cholesterol will settle within it, it tends to settle within non-scarred areas. Occasionally, it also settles in areas around the area previously treated.
If your scar is more prominent it is very important to be patient and wait for up to 2 years as well as do the aftercare interventions we recommend to you to minimise scarring. Many scars will get better and better over time and slowly contract and turn from pink to white.
Who is more likely to be unhappy with the outcome
In our experience the least likely patients happy with the outcome is young women (sometimes exacerbated by mental health conditions like depression), whose confidence is extremely affected by the Xanthelasma and / or who want a perfect result. This is particularly the case if the scar is not settling as quickly as they hoped to. We would recommend ladies under 45 years of age with taut skin to be very careful before choosing any service or any treatment including our service.
Another group of patients that is sometimes not so happy are more dark skinned patients, who choose the Electrodessication method. We often find that Cholesterol in dark skinned patients is deeper located and often recommend excision in those patients. A scar in dark skinned patients can be lighter and the contrast higher compared with surrounding skin. Also darker skinned patients have a higher return rate for Cholesterol due to their underlying genetics and it is even more important to look at Cholesterol lowering measures wherever possible.
Who is likely to be happy with the outcome?
The large majority of patients are very happy with the outcome. Women often prefer a scar as it is easier to cover with make up than the bright yellow Cholesterol. Men tend to prefer it, because men often do not worry about scars as much than about the bright yellow signal colour of cholesterol in the eyelid (no a universal truth, but a common one). Generally the face is a region that is exposed to air and weather and tends to heal well. For example a man shaving and cutting himself does not usually end up with a permanent scar.